The Integrative Cancer Resource Society trademarked the POWERMEETS series and partnered with cancer foundation leaders to spearhead new meetings about dense breast education advocacy and breast cancer awareness. Together, they form a collaborative alliance to expand the reach of their common message and make a wider difference in the process.
In Sept. 1, 2023, a collective Powermeet hosted by Mr. Joe Cappello (founder of "Are You Dense?") was aired to welcome Ms. Allie Fiederlein to the national advocacy movement for dense breast and breast cancer awareness. She is recognized as "the voice for her generation" of the underserved and underdiagnosed women (ages 20-39). Together with the ICRS, Ms. Fiederlein is part of the campaign aptly called "EARLIER DETECTION". Notable speakers from live conferences, pre-recorded testimonies and emailed supportive statements were published in this special event- brought to you in part by "Are You Dense?" Foundation.
MEMORABLE STATEMENTS FROM THE 9/1 POWERMEET
JOE CAPPELLO: Allie! It's great to have you on board because you represent a
multitude of new patient groups. When
we're talking about cancer detection for a younger generation, it is amazing how many
people you're gonna affect. And your voice is very important for our mission. It's something to to behold because there's not
a lot of strong women like yourself who's willing to step out and represent a
vast majority of women who are hurting, but are afraid to come forward and
maybe not even know. But the assumption is that they should
know... and that's your voice! We've come a long way with "Are you Dense?" We do a lot off shooting in the dark, not
knowing which way to go- but in the end, we
knew we're making progress for the last 20 years. All we do
is to keep moving forward. (See: Joe Cappello's feature on Dense Breast Legislation 2023)
NOELLE CUTTER, PhD: Allie- I am so very proud of you, not just because you were one of my top students @ Molloy (University) but because you were always an achiever- deserving off this honor. Today, you're one of us (national advocates) and I want to be the first to congratulate you for this honor. Being a spokesperson for young women in your age group is truly a milestone for addressing the age barrier about a generation in crisis. Breast cancer is the most common cancer worldwide, recently surpassing lung cancer in 2020. The median age of diagnostics is 62 to 63 years old, but more recent data also shows that breast cancer is the most common type of cancer among young women. Ages 15 to 39 accounting for 30% of all cancers in this age group, understanding both the genetic and environmental makeup of the cancer will help drive better treatment for our patients. (See Dr. Cutter's report on "Ultrasound Significantly Reduces False Readings of DENSE BREASTS")
ALEXANDRA (ALLIE) FIEDERLEIN: My generation is the most underserved when it comes to education and awareness- and also the most underdiagnosed. Where the vast majority of the younger women have dense breasts, a great unknown number of them are potential breast cancer cases because of this- but no one has that data because mammograms don't happen as a standard until 40. Thanks to this collaboration technology (web & video conferencing), we have the advantage to reach everyone out there more easily. We're called GEN-Z... and that's the best thing about reaching my generation because everyone on my end is on Instagram, on Twitter, Facebook-- essentially web-connected. It's a whole new world that we can access and we
have to know how to use it effectively in that manner. My interest is to reach out, engage and offer true awareness to the younger women- the underserved women who have no idea about GETTING CHECKED NOW! (See Allie's spotlight feature on Earlier Detection)
ROBERT BARD, MD: Speaking of generations, for us to help the underserved, we need to educate the older generation of doctors who are by and large not particularly interested in change. Use of non-invasive imaging technologies like 3D ultrasound and elastography are coming up to greatly help with early detection- instead of just a mammogram. There's an interesting link between dense breast and inflammatory disease and cancer. Meanwhile, we need more data on breast cancer cases within the younger women's age group (20-39) and there isn't any because there's no real push to get a mammo for this generation. With people like ALLIE speaking out about getting more screening, you'll find that data drive a shift in attitude as far as early detection for her age group! (See Dr. Bard's report on "The Risk of Being "Too Young for a Mammogram")
ROBERTA KLINE, MD: Since its inception, this group has always amazed me with its vision to unite change-makers and visionaries. After all, cancer is not won from one battle front but from many. Now, we are clearly seeing an age group in crisis where cancer continues to rise simply because of a lack of attention. Allie's age group is actually first to be affected because of a lack of education and awareness, compounded by the socio-political challenges of insurance coverage and outdated practice guidelines for the medical community that perpetuate the belief that breast cancer does not happen under 40. Of course, this is far from true- but (like Dr. Bard mentioned), it's the DATA that the world listens to. So, if everyone subscribes to a data-driven approach with regular screening and personalized care, we'll change course for Allie's generation. Congratulations, Allie-- welcome to the fight! We are with you! (See Dr. Kline's report on Epigenetic Research & Profiling the Dense Breast Paradigm)
M.J. SMITH: Earlier detection sounds in line with my personal and professional missions. If I could wave a magic wand right now and make one single change to how we look for breast cancers, it would be to get, every woman to have a baseline mammogram at age 20. And then, in different intervals, depending on family history and breast density, 40 is that age where starting screening was established. We don't have real information available when young women may actually get breast cancer? It's devastating. They're often sent away saying, "you know, you felt this lump... you're too young to get breast cancer". There's definitely a perception issue in the medical community because of the organizations that are giving them these guidelines-- and insurers are paying only starting at age 40. There's also some exciting information coming out of AI applied to mammography and ultrasound, which are two ways that you can screen for breast cancer. AI is also helping us to determine which types of that tissue are more risky. (See MJ's spotlight video interview on Women's Health Digest about Earlier Detection)
Under a joint report with the Women's Diagnostic Network and HealthTech Reporter, our editors caught up with Ms. MJ Smith, a clinical ambassador from Screen Point Medical (breast imaging AI) at the 2023 NYC Roentgen Society conference. At the height of the medical conference, we found MJ to be a uniquely profound and engaging speaker about women's health topics. Exploring a private connection opened us into a collaborative and educational journey befitting our UNDERDIAGNOSED WOMEN series where MJ is truly a life-long crusader in support of clinical advocacy.
Endometriosis (sometimes called "endo" for short) is a common health problem in women that is reported to affect more than 11% of American women between 15 and 44. It gets its name from the word endometrium, the tissue that normally lines the uterus or womb. When this tissue is found in locations outside of the uterus, it is called endometriosis. Most often this involves the nearby organs and tissues – ovaries, fallopian tubes, outer surface of the uterus, bladder, bowel and rectum. It can also be found in other locations including the vagina, cervix, vulva, or even distant tissues such as the lungs, brain, eye, and skin. Just like the lining of the uterus, this tissue responds to cycling hormones to grow. But unlike normal endometrium, it is not limited to the surface and does not shed. Because of this, it builds up and creates inflammation, scarring, and other changes that contribute to the most common symptom: pain.
While endometriosis is most often diagnosed in women in their 30s and 40s, it likely develops much earlier. Due to the wide range of symptoms that women can experience, and lack of effective and noninvasive diagnostic tools, women often suffer for years or even decades. Currently the only accepted way to diagnosis endometriosis is to directly visualize and biopsy the lesions with surgery. This is limiting for two reasons. First, endometriosis has to be considered as a possible explanation for symptoms that are often seen as “normal” for menstruating women. Second, the risk of not knowing has to outweigh the risk of potential complications of invasive surgery.
Endometriosis can also make it harder to get pregnant, and it is not uncommon for a diagnosis to be made only as part of evaluation or treatment for infertility. Getting a diagnosis to explain symptoms is only the first step in addressing endometriosis, however. There is no cure, and most current treatments often come with significant risks or side effects but do not fully resolve a woman’s symptoms. While research progresses slowly, we still do not have a clear understanding of what causes endometriosis, how to diagnose it early without invasive procedures, how to ease symptoms, and ultimately treat and possibly cure the disease itself.
This special interview features great insight from a woman’s journey with endometriosis. We explore her remarkable quest for answers from the range of pain relief to therapeutic treatments to risks of surgical solutions.
LIVING WITH ENDOMETRIOSIS: From an interview with MJ Smith
My personal and professional missions are both in women's health. By day, I work for a breast AI company focused on helping radiologists find breast cancers on mammograms. I chose this path because I believe in advancing causes that support women's health simply because women are core members of our culture and our families. I have had two family members, both maternal aunts, who died of breast cancer, - one at the age of 36, and an the other at the age of 52.
Advocacy for Endometriosis is directly related to my personal journey. Growing up with endometriosis since puberty, I've been to the emergency department probably over 20 times for pain or pelvic pain related conditions. The pain had me flat on my back for days at a time or falling out of bed with pain. I drove myself to a Planned Parenthood in Minnesota where I grew up and was prescribed birth control to manage it well into my twenties. Despite the hormonal treatments, I still had a series of episodes.
Endometriosis is the uterine tissue that grows and implants itself outside of the uterus. Going through that pain is the result of a complex process, resulting in swelling and bleeding inside the interstitial spaces of my body. Women who have endometriosis also often develop painful cysts on their ovaries.
I think the biggest reason you see women in the ER is pelvic pain. Women with chronic pelvic pain (which is often what endometriosis causes) are underserved by the healthcare community because we're constantly complaining of pelvic pain. The ER is not where you want treatment because you see a different doctor every time you get admitted. With emergency imaging, you usually get a pelvic ultrasound where cysts can show up and they're quick to assume that you have a cyst, or a cyst has burst and this is why you're uncomfortable. I think now you can do a pelvic MRI with contrast media- but it's still not enough to offer a definitive diagnosis. (To be continued below)
ULTRASOUND DIAGNOSTICS OF ENDOMETRIOMA
ENDOMETRIOSIS REVIEW 2023: FROM ESSENTIALS TO ADVANCEMENTS
According to the World Health Organization, Endometriosis
affects roughly 10% (190 million) of reproductive age women and girls globally.
It is a chronic disorder that can result
in life-disrupting pain during menstrual periods, sexual activity and urination. Currently, there remains no known cure for
endometriosis, whereby treatment is usually aimed at managing its known
symptoms. One objective of the medical
community is to conduct early diagnosis and research continues to pursue effective
treatments.
Endometriosis starts in the endometrium with abnormal
cellular proliferation. Through the use
of 3D Ultrasound, this disorder can be measured through the monitoring of the
widening or the increased tissue in the endometrium. Another form of quantitative measure is by the
study of blood flow in the endometrium. Its ability to spread can be recognized
by the number of vessels in the active tissue. The big problem with staging endometriosis (or
endometriomas) are the cysts that follow it.
Because of its capacity to spread in most areas of the body, a strategic
protocol for clinical management is to conduct IMAGE GUIDED treatments, whereby
use of real-time scanning of or during therapeutic process helps navigate the
focus the treatment area. Imaging
solutions include CT (which has radiation), MRI, or the 3D Doppler ultrasound.
CASE REVIEWS: We recently had a case where the endometriosis had
metastasized under the arm. We've seen it metastasize in post-op scars. We can
see the endometrial tissue block the ureters- hence, blocking the kidneys and
destroying the kidney function. Moreover,
the scars can cause bowel obstruction.
While it's not categorized as malignant, it certainly can
be deadly (as well as a seriously painful and debilitating disease). Women (especially
those in advanced age groups) have expressed being completely incapacitated for
three out of four days during their menstrual cycle.A vast majority of them also claimed
experiencing mental health issues because of the pain and discomfort.
The following slides are from Dr. Robert Bard's lecture presented in 2016 for the obstetrics and gynecology department at Mount Sinai Medical Center in New York City (ref: prior lecture from Harvard Medical School/the American Institute of Ultrasound in Medicine).
Use of the modern image guided treatment technologies offer non-invasive blood flow technology, which quantifies the aggression, either the aggressiveness of an inflammatory process like endometriosis or the invasive and metastatic potential of cancers such as endometrial cancer & cervical cancer.
FIG 1: Upon observation, this it is not a primary bladder cancer.
This is an inflammatory mass because the vessels are smooth (cancer vessels are
wrinkly)- and there is a visible difference between the two. This is a three dimensional pelvic floor doppler study of the pelvis. If we start with scan A, we see the uterus on the bottom half and the bladder on the top, which is black, and within the black fluid is a mass. By looking below that, we see the (scan C and D) the abnormal blood vessels of the endometriosis. Hence, inflamed tissue is vascular and the same pattern of blood vessels from the abnormal endometrium is also in the bladder, indicating that the endometrial tissue has either invaded or metastasized into the base of the bladder. The two scans (B & D) show the bladder wall is intact. Hence, these are endometriosis that has metastasized or spread to the base of the bladder.
FIG 2: In this image set, we have an endometrioma, which is (again) a large black area where the fluid is black, and within it, there's another nodule with the circle indicated by the red highlight. We see that there's no blood flow in this- hence, it's not a primary cancer of the bladder. In addition, it is not particularly active inside the bladder, however, there is a stalk that is feeding blood vessels to the cystic area. With the 3D Doppler, we can quantify the cyst in seconds, because 3D takes a dataset in 15, 20 seconds of a hundred, 150 pictures of the whole area, including the blood flow.
Notice the 3D images on the left with the red circle (Scan A) is the endometrial cyst, which is black, and the circle shows a small nodule within the cyst. What's important with this as contrasted to the previous study is this is NOT VASCULAR, which means this is inactive or subclinical at this time. On the right (E,F,G,H), we see that the pedicle that's going to the cyst and feeding the cyst, the area has multiple blood vessels in it. Because we're using 3D volumetric technology, we are able to quantify the number of vessels in the pedicle. The more blood vessels in the pedicle, the more aggressive the disease is. So back to the cyst. The cyst, there were no vesicles, but the pedicle feeding the cyst had a 13% ratio of blood vessels to assisted tissue.
EPILOGUE
Traditional medicine has not assisted with the mental depression, the anguish of the certainty that the pain will be monthly and the possible side effects including infertility. Since we've been using targeted therapies with lasers and focused ultrasound energies years ago, we are now globally using bioenergy treatments that is the near infrared laser and the pulse electromagnetic fields to calm down the, the inflammatory process of this inflammatory disorder.
(MJ Smith: Advocate's Journal- CONTINUED)
I found in the 20 years of suffering endometriosis that the only way to get a true diagnosis has remained to be a laparoscopic or an open pelvic surgery. It's incredibly difficult.
I know another woman who struggled through over seven years of infertility and it was only after seven years, and by then she was well into her late thirties or early forties, that she had surgery to identify endometriosis. Only then was that woman able to get pregnant. I have had a similar experience. I wasn't suffering infertility, but I was in so much pain in my late twenties that my doctor recommended a laparoscopic exploratory surgery because the pain is was so severe. I remember I was prescribed a month's worth of Vicodin leading up to the surgery. I am not a person who developed an addiction to pain medicine- but in retrospect this was done in the time when the entire country fell into a pandemic of addiction to pain medicine. I wouldn't have gotten that prescription in this day and age in 2023 if I have pelvic pain. Overall, there's no relief for me and over-the-counter meds that do not help. I just thank God I didn't develop an addiction after having taken Vicodin multiple times a day for a month leading up to that surgery... where, in fact, I was diagnosed with stage four endometriosis.
One of my ovaries was almost lost due to endometriosis. My doctor was able to keep that ovary and as a result I was able to get pregnant with my first child. I had a second child years later but surgery comes with complications. To this day, at 44, I recently went to the emergency department because of pelvic pain and it's still something I live with. I do take hormones but I've given up on looking for answers from academic research because I think that, in my opinion, I don't think we've gotten very far. The choice of hormones have side effects like an increased risk of breast cancer or uterine cancer. I'm very interested in minimally invasive treatment procedures but I just think we've come to a standstill with the traditional medical community when it comes to endometriosis.
SEXISM IN THE WOMEN'S HEALTHCARE
by: Mary Nielsen
Many women suffer with undiagnosed endometriosis. The medical field has prided itself on providing objective observations because it claims to rely on science. However, sexism lurks in hospitals, clinics and other health care facilities and the gender gap in treating pain is real. Diane Hoffman and Anita Tarzian from the University of Maryland, Francis King Carey School of Law published, "The Girl Who Cried Pain, A Bias against Women in the Treatment of Pain." Although that study is 20+ years old, little has changed.
Sexist stereotypes that see women as 'emotional' and consequently medical staff doubt a physical basis for women's pain. Men are viewed as more 'rational' and when men say they are feeling acute pain, their symptoms are taken more seriously and considered to have a physical cause. This means women receive very different care for pain management and pain diagnosis. Researcher, Karen Calderone found that women are more likely given sedatives as an answer to complaints of pain and are perceived as being anxious.
Medical professionals focus on returning the woman to a state of being calm and not investigating the cause behind their pain. The sedatives can then make the women seem calmer from outside appearance, while their medical condition can continue to worsen as they remain undiagnosed. Undiagnosed endometriosis has enormous repercussions for a woman. Life altering heavy bleeding, cramping and pain can lead to infertility, anemia, and internal adhesions requiring surgery.
Education toward gender bias and addressing women's pain is needed to allow earlier diagnosis with a non-invasive technology like ultrasound.
MARY NIELSEN (Founder/ Faculty Director - Spectrum Advanced Aesthetics)
Mary established and manages a certified aesthetics institution in Portland Oregon supporting the academic leadership and technical ability to grow a med spa profitably. Through collaborative relationships with evolving aesthetics business, her programs (Fearless Beauties and Cascade Aesthetic Alliance) functions to help the esthetician, whether newly licensed or a veteran with education and networking. She is also a published author of best selling textbooks in aesthetic wellness including ADVANCED AESETHETICS and FEARLESS BEAUTIES. Mary is dedicated to bringing change to the esthetics/beauty industry through comprehensive education and empowerment through knowledge. https://www.fearlessbeauties.org/
CONTRIBUTORS
BOBBI KLINE, MD (Educational Dir. /Women's Diagnostic Group)
Dr. Kline is a board-certified ObGyn physician, Integrative Personalized Medicine expert, consultant, author, and educator whose mission is to change how we approach health and deliver healthcare. She helped to create the Integrative & Functional Medicine program for a family practice residency, has consulted with Sodexo to implement the first personalized nutrition menu for healthcare facilities, and serves as Education Director for several organizations including the Women’s Diagnostic Health Network, Mommies on a Mission. Learn more at https://bobbiklinemd.com
ROBERT L. BARD, MD (Diagnostic Imaging Specialist)
Having paved the way for the study of various cancers both clinically and academically, Dr. Robert Bard co-founded the 9/11 CancerScan program to bring additional diagnostic support to all first responders from Ground Zero. His main practice in midtown, NYC (Bard Diagnostic Imaging- www.CancerScan.com) uses the latest in digital Imaging technology has been also used to help guide biopsies and in many cases, even replicate much of the same reports of a clinical invasive biopsy. His most recent program is dedicated to the reporting of mental health diagnostic and innovative solutions including the use of modern neuromagnetic technologies and protocols in his MEDTECH REVIEWS program.
2024 CLINICAL PROFILE OF THE DENSE BREAST PARADIGM - for the Obstetrics & Gynecology Society
Breast cancer affects the lives of hundreds of thousands of women every year and is a leading cause of death. While we have made great progress in advancing earlier diagnosis and more individualized treatments, we still need to improve our approach to achieve our ultimate goal - prevention. This requires a deeper understanding of the molecular mechanisms and the multitude of factors that contribute to the development of breast cancer.
Dr. Roberta Kline, recognized speaker and publishing crusader for women's health brings you a comprehensive review and a deep-dive analysis of the current research findings about breast density and its major risk factors for breast cancer. Her reports uncover current imaging practices and clinical protocols updated in great support of breast density detection and the means of addressing this growing condition that affects over 45% of the female population. "Knowing a woman has greater breast density is a critical first step, but it doesn’t end there... we need to go further by understanding the causes of breast density, and how they relate to breast cancer-- we now have another avenue to proactively intervene to reduce risk or even prevent breast cancer in the first place." This textbook is a champion in targeting the Dense Breast Paradigm as a blueprint and a clear course study for all clinical professionals who are dedicated to women's early detection and prevention programs. (More information)
LAUNCHING IN 2024: NATIONAL COALITION OF WOMEN'S HEALTH SUPPORT
Professional health orgs, foundations and advocates of women's health disorders (primarily cancers) is uniting to form a national alliance of collaborators. This collective group is focused on "doing more together" as far as exploring new resources, sharing current ideas and addressing a wide range of topics about women's issues. Meetings like our latest Women's Powermeet series discussed the latest in diagnostic and therapeutic solutions while introducing who's who in national crusadership in the advocacy realm. Clinicians are also welcome to discuss patient-dedicated road maps and a more thoughtful health analysis and research-based evaluation. It is this level of commitment to women's health that provides a deeper sense of care for the patient that lends itself to a more holistic and integrative strategy to therapeutics. It is also this philosophy that draws more intuitive and insightful awareness on a global scale to offer collaboration platforms too better share insights on a patient's disorders to seek out better solutions. (See Women's Health Digest)
WOMEN’S HEALTH DIGEST
From the publishers of THE WELLNESS JOURNAL and the WOMEN'S DIAGNOSTIC NETWORK NEWS comes a consortium of IPHA'S top professional contributors in women's health & wellness advocacy. Subscribe to our latest community E-news forum and get the insiders news on pain therapeutics, diagnostics and lifestyle upgrades. We welcome special guest contributors from all modalities of healing - from practitioners, product innovators and researchers. Also, gain valuable insight from success stories of real people and their experience with WHAT WORKED for them! Get front row access to our latest headlines. Visit: WomensHealthDigest.org
Health issues are often linked to a range of emotional distress, but a major contributor to the progression of chronic issues such as urinary incontinence starts with the sufferer's instinct to conceal the problem. This reactive response from embarrassment and shame drives many women (both men and women) to hide their condition from their closest supporters as well as their physicians, making incontinence go unchecked and unaddressed. Over time, it is this level of clinical neglect that brings bladder health issues and urinary incontinence to grow into a more challenging health condition.[1]
Internalizing reactive shame plays a critical role in the effects of STIGMA and its self-propelling negative cycle, further driven by self-esteem issues, depression and hopelessness. From a 2002 World of Psychiatry report, both public and self-stigma may carry three components: stereotypes, prejudice, and discrimination. These elements are observed to be quite powerful in driving human activity and decision-making as they align with our sense of social acceptance, personal safety and survival.[2]
There have been many studies evaluating groups of sufferers of urinary incontinence directly reflecting emotional distress. Under varying conditions of functional loss, the investigative teams in these studies tend to conclude similar association between this physical impairment and levels of anguish and anxiety where the embarrassment of incontinence would often lead to self isolation- where seeking direct care or proper counsel is often compromised.[3]
INTRODUCTION: In my experience as an ObGyn, urinary incontinence is the unspoken secret among women. It affects up to 1 in 4 women, and this increases with age so that by age 65 up to 75% of women are affected [1]. And yet, most women never seek help. In a study published in 2013, 95% of women reported a negative impact on their quality of life, and yet 64% of the women had never received any medical help [2]. So often hidden out of shame, many women suffer in silence despite many efforts to raise awareness. Even those that are aware there is help may not seek it. What’s the point of speaking up when you fear it will only lead you down a path full of embarrassing conversations, invasive testing or procedures– and often does not produce effective or long-lasting results?
THE 'UNSPOKEN FEMALE DISORDER' While urinary incontinence is most common in women over age 50, it can happen to women of all ages. More recent research is also showing that ethnicity plays a role. Sometimes the cause is temporary, as can happen with a urinary tract infection. Pressure on the bladder, as we see in pregnancy or from fibroids or other pelvic masses, can also lead to incontinence. Addressing the underlying issue typically leads to resolution of the urinary leakage.
But most commonly, the involuntary loss of urine is not so easily fixable. The causes of urinary incontinence are grouped into four different categories: urgency, stress, functional and overflow incontinence. Functional and overflow incontinence are typically due to non-bladder related causes, while urgency and stress incontinence are closely linked with dysfunction of the bladder or other structures in the pelvic floor.
The bladder is a sac made up of smooth muscle, and when it fills up with urine there is a reflex that results in release of that urine. Early in life we learn to control when those muscles contract, and thus control when we urinate.
URGENCY INCONTINENCE occurs when there is some loss of that control (3). This is often called “overactive bladder”, or OAB. Certain substances, such as caffeine or wine, or changes in hormones related to menopause, are known to aggravate this. But most often, we don’t know why this occurs. As a result, lifestyle or medication treatments are often less effective because we aren’t addressing the root cause.
STRESS URINARY INCONTINENCE is most often caused by trauma to the pelvic floor during childbirth, when the muscles that are designed to support the bladder are weakened (3). As a result, women leak urine when the bladder is put under pressure such as with coughing, sneezing, laughing or jumping. This is fairly common immediately after vaginal delivery, and many women will notice their symptoms improve with Kegel exercises designed to strengthen these pelvic floor muscles, along with the natural healing process. In my experience, many women are not sufficiently educated and supported in this. Or, as is especially the case with new moms, they are so busy taking care of everyone else that they neglect their own health needs.
Some women never fully recover, and even those that do often see the stress incontinence symptoms return later in life. And to make things even more challenging, often women have both urgency and stress incontinence. So women hide, often arranging their whole lives around avoiding leaking urine because they are ashamed to seek help. They change their exercise routine. They forego activities that bring them joy and pleasure, including sex. They buy pads and hope no one notices. They are always worried about a leak that reveals their shameful secret.
In my opinion, it’s part of a larger problem in how we view and treat women’s bodies. But fortunately, things are starting to shift thanks to technological advances in both our understanding and treatment. Even Personalized Medicine is yielding breakthrough insights into underlying causes. We are learning how each woman’s DNA related to pelvic floor muscles and collagen, and the DNA of her urinary microbiome, can impact her risk as well as the effectiveness of current treatments.
I am optimistic we may someday soon be able to truly tailor both prevention and treatment in a way that is much more accessible and effective in addressing urinary incontinence in women.
Why I wear Pull-Ups… By: Jesi Stracham
When Depends became too baggy after my weight loss causing leaks and the pads would slide to the side, I switched to GoodNites brand children’s diapers. Immediately, my confidence was boosted with the cute designs and panty like fit. Even though I have my bladder well managed, I still wear them daily. With my active lifestyle I like the piece of mind that if I have an accident my wheelchair cushion and clothes will still be dry. I simply rip the diaper off, clean my downstairs “area” with a baby wipe, put a new diaper on and wheel on my way.
Often times SCI survivors suggest Botox Injections and pharmaceuticals to help with my incontinence. I used both up until April 2017 when they quit working. I searched high and low for natural alternatives after realizing how well my body felt after getting off of the pharmaceuticals. The uncomfortable constipation and dry mouth ceased within days!
Early summer 2018 I had a bladder study done. The nurse who perform the study shamed me for refusing to take the prescribed medicines. She put me in tears saying due to the amount of spasms my bladder has shrunk significantly. She continued on with a shame train because I refused pharmaceuticals after explaining they didn’t work and made me feel funny. She placed fear deep within my soul threatening that I would need a permanent catheter in my stomach with a bag or bladder augmentation (surgery where they take a piece of your bowel to make you bladder bigger) before I knew it. (see complete Blog entry)
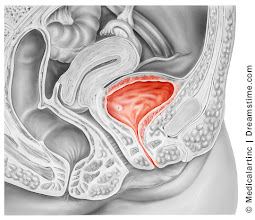
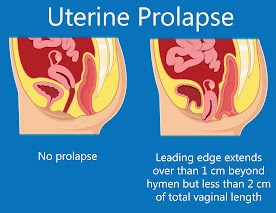
Prolapse of the pelvic floor contents (the uterus, bladder or the anus) is also associated with incontinence. 3-D pelvic floor ultrasound is performed in two ways:
1) transvaginal probe which goes inside the vagina
2) transperineal scan which is a more common way for evaluating stress urinary incontinence since the trans perineal probe is applied at the outside of the pelvic floor in the area between the vagina and the anus which is called the perineum.
MRI has been used for years to image the prolapse of the pelvic organs but is being replaced by the 4D real time transperineal sonogram as it is quicker and instantaneously shows the tear in the muscular ring (levator sling) that is associated with the trauma of birth. This exam is done in the privacy of an office instead of an MRI center or hospital setting and may be completed in a few minutes by the physician or specially trained technician. The muscle bundle that supports the bladder is white on the sonogram while the tear is black and readily distinguished. During the examination the patient participates actively by bearing down or straining (Valsalva maneuver) to provide an exact measurement of the degree of the descent of the uterus, urethra, bladder or rectum.
THERAPY
Stress urinary incontinence (SUI) is distinct from overactive bladder (OAB) while both may be problematic in older patients with weaker muscle tone. The KEGEL maneuver is a common therapeutic approach to improve muscle strength and diminish the loss of urine when coughing, sneezing or laughing. While the technique is simple, the learning curve is often difficult for women who are accustomed to bearing down rather than “sucking up” the anus or vagina. While 4D ultrasound is optimal for diagnosing the cause, it is sophisticated equipment and requires advanced medical skills. It can go beyond diagnosis and aid in treatment: the demonstration of the bladder change in the proper Kegel contraction is visible to the patients as a dynamic training guide by the physical therapist.
The bladder descends during the Valsava while the bladder and urethra move upward in the correct maneuver. This equipment is portable so it may be brought to the patient rather than a clinic visit or a treatment facility. The technology is also wireless and point of care (POC) images may be transmitted to a reading site for interpretation as is done in ambulances where the EKG is read remotely by the Emergency Department physician while the patient is in route.
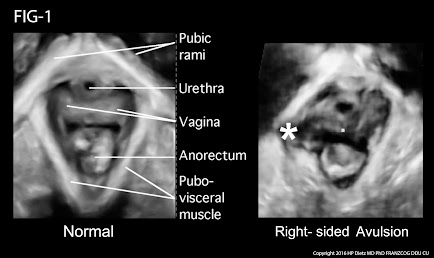
FIG-1: Postpartum delivery and difficult childbirth are a major cause of pelvic floor trauma, muscle tears and of course, urinary and fecal incontinence. The ovoid white muscular ring in this case on the right shows a star, which indicates that the white muscular lining, which is smooth on the right hand side of the picture is bulging and actually torn and disappeared by a black area, indicating the exact location at the extent of the tear. This is important preoperatively for reconstructive pelvic floor surgery. While the 3d probe takes 15 seconds to scan the entire pelvic floor surface, it takes training and of course the specialized ultrasound technology, which shows the location and the depth of the disease. More importantly, the patient dynamically assists that is active patient participation to bear down or Valsalva or hold the urine for a varied period of time is important for measuring the descent of the bladder and the uterus in the pelvic floor. Thank you very much for your attention.
For the reasons of accurate diagnosis and ease of use, pelvic floor ultrasound is widely used in Europe and becoming popular in the US. The technology is safe and a “black and white” visual aid for learning the Kegel maneuver. Additionally, during the diagnostic evaluation, the physician will look for other etiology of the voiding dysfunction such as bladder stone, bladder cancer and cystitis as well as inflammatory urethritis which is seen with treatments such as transvaginal tape (TVT) or surgical devices that are implanted. Complications of endometriosis and cervical, ovarian or uterine tumors may be detected and definitive treatment may be timely instituted.
Reference:
Dietz, H.P., Pelvic Floor Ultrasound Ultrasound, Atlas and Textbook , 2016 Obstetrics and Gynaeoclogy- Springwood NSW Australia
CONTRIBUTORS
BOBBI KLINE, MD (Educational Dir. /Women's Diagnostic Group)
Dr. Kline is a board-certified ObGyn physician, Integrative Personalized Medicine expert, consultant, author, and educator whose mission is to change how we approach health and deliver healthcare. She helped to create the Integrative & Functional Medicine program for a family practice residency, has consulted with Sodexo to implement the first personalized nutrition menu for healthcare facilities, and serves as Education Director for several organizations including the Women’s Diagnostic Health Network, Mommies on a Mission. Learn more at https://bobbiklinemd.com
ROBERT L. BARD, MD (Diagnostic Imaging Specialist)
Having paved the way for the study of various cancers both clinically and academically, Dr. Robert Bard co-founded the 9/11 CancerScan program to bring additional diagnostic support to all first responders from Ground Zero. His main practice in midtown, NYC (Bard Diagnostic Imaging- www.CancerScan.com) uses the latest in digital Imaging technology has been also used to help guide biopsies and in many cases, even replicate much of the same reports of a clinical invasive biopsy. His most recent program is dedicated to the reporting of mental health diagnostic and innovative solutions including the use of modern neuromagnetic technologies and protocols in his MEDTECH REVIEWS program.
JESSICA CONNELL-GLYNN, LCSW, CPC, CEC - (Mental Health Dir.)
As a therapist and mental health coach for the Women's Diagnostic Network, Jessica's expertise is highly in-demand in many areas of pre/post procedural care. She provides direct support in managing personal anxiety, panic, targeting TRAUMA and residually related fear. This is specialized work honed by her extensive experience and research with the general public and within the Women's Wellness community. Jessica is also currently leading an interdisciplinary research project with a team of mental health and professionals in neurology, assessing psychological disorders. (Visit her website- www.jagtheracoach.com
JESI STRACHAM is a trauma survivor on a mission to help individuals see the opportunity in their obstacles. She is the founder of Wheel With Me Foundation, the owner of Wheel With Me Consulting, and a fitness and growth coach. Through her struggles, she works for teaching individuals the power of our mindset. Jesi is an honest, authentic, America-loving athlete. Over the past several years, she has generated a significant following among both the spinal cord injury and able-bodied community. Her goal is simple: show the world there is an opportunity in their obstacles, restoring hope during life’s difficult moments. She helps people achieve their dreams through the importance of goal setting, taking control of what we have control over, and showing YOU what’s possible with consistent hard-work.
2024 CLINICAL PROFILE OF THE DENSE BREAST PARADIGM - for the Obstetrics & Gynecology Society
Breast cancer affects the lives of hundreds of thousands of women every year and is a leading cause of death. While we have made great progress in advancing earlier diagnosis and more individualized treatments, we still need to improve our approach to achieve our ultimate goal - prevention. This requires a deeper understanding of the molecular mechanisms and the multitude of factors that contribute to the development of breast cancer.
Dr. Roberta Kline, recognized speaker and publishing crusader for women's health brings you a comprehensive review and a deep-dive analysis of the current research findings about breast density and its major risk factors for breast cancer. Her reports uncover current imaging practices and clinical protocols updated in great support of breast density detection and the means of addressing this growing condition that affects over 45% of the female population. "Knowing a woman has greater breast density is a critical first step, but it doesn’t end there... we need to go further by understanding the causes of breast density, and how they relate to breast cancer-- we now have another avenue to proactively intervene to reduce risk or even prevent breast cancer in the first place." This textbook is a champion in targeting the Dense Breast Paradigm as a blueprint and a clear course study for all clinical professionals who are dedicated to women's early detection and prevention programs.(More information)
LAUNCHING IN 2024: NATIONAL COALITION OF WOMEN'S HEALTH SUPPORT
Professional health orgs, foundations and advocates of women's health disorders (primarily cancers) is uniting to form a national alliance of collaborators. This collective group is focused on "doing more together" as far as exploring new resources, sharing current ideas and addressing a wide range of topics about women's issues. Meetings like our latest Women's Powermeet series discussed the latest in diagnostic and therapeutic solutions while introducing who's who in national crusadership in the advocacy realm. Clinicians are also welcome to discuss patient-dedicated road maps and a more thoughtful health analysis and research-based evaluation. It is this level of commitment to women's health that provides a deeper sense of care for the patient that lends itself to a more holistic and integrative strategy to therapeutics. It is also this philosophy that draws more intuitive and insightful awareness on a global scale to offer collaboration platforms too better share insights on a patient's disorders to seek out better solutions. (See Women's Health Digest)
Disclaimer: The information (including, but not limited to text, graphics, images and other material) contained in this article is for informational purposes only. No material on this site is intended to be a substitute for professional medical advice or scientific claims. Furthermore, any/all contributors (both medical and non-medical) featured in this article are presenting only ANECDOTAL findings pertaining to the effects and performance of the products/technologies being reviewed - and are not offering clinical data or medical recommendations in any way. Always seek the advice of your physician or other qualified health care provider with any questions you may have regarding a medical condition or treatment and before undertaking a new health care regimen, never disregard professional medical advice or delay in seeking it because of something you read on this page, article, blog or website.


 NOELLE CUTTER, PhD: Allie- I am so very proud of you, not just because you were one of my top students @ Molloy (University) but because you were always an achiever- deserving off this honor. Today, you're one of us (national advocates) and I want to be the first to congratulate you for this honor. Being a spokesperson for young women in your age group is truly a milestone for addressing the age barrier about a generation in crisis. Breast cancer is the most common cancer worldwide, recently surpassing lung cancer in 2020. The median age of diagnostics is 62 to 63 years old, but more recent data also shows that breast cancer is the most common type of cancer among young women. Ages 15 to 39 accounting for 30% of all cancers in this age group, understanding both the genetic and environmental makeup of the cancer will help drive better treatment for our patients. (See Dr. Cutter's report on "Ultrasound Significantly Reduces False Readings of DENSE BREASTS")
NOELLE CUTTER, PhD: Allie- I am so very proud of you, not just because you were one of my top students @ Molloy (University) but because you were always an achiever- deserving off this honor. Today, you're one of us (national advocates) and I want to be the first to congratulate you for this honor. Being a spokesperson for young women in your age group is truly a milestone for addressing the age barrier about a generation in crisis. Breast cancer is the most common cancer worldwide, recently surpassing lung cancer in 2020. The median age of diagnostics is 62 to 63 years old, but more recent data also shows that breast cancer is the most common type of cancer among young women. Ages 15 to 39 accounting for 30% of all cancers in this age group, understanding both the genetic and environmental makeup of the cancer will help drive better treatment for our patients. (See Dr. Cutter's report on "Ultrasound Significantly Reduces False Readings of DENSE BREASTS") ALEXANDRA (ALLIE) FIEDERLEIN: My generation is the most underserved when it comes to education and awareness- and also the most underdiagnosed. Where the vast majority of the younger women have dense breasts, a great unknown number of them are potential breast cancer cases because of this- but no one has that data because mammograms don't happen as a standard until 40. Thanks to this collaboration technology (web & video conferencing), we have the advantage to reach everyone out there more easily. We're called GEN-Z... and that's the best thing about reaching my generation because everyone on my end is on Instagram, on Twitter, Facebook-- essentially web-connected. It's a whole new world that we can access and we
have to know how to use it effectively in that manner. My interest is to reach out, engage and offer true awareness to the younger women- the underserved women who have no idea about GETTING CHECKED NOW! (See Allie's spotlight feature on Earlier Detection)
ALEXANDRA (ALLIE) FIEDERLEIN: My generation is the most underserved when it comes to education and awareness- and also the most underdiagnosed. Where the vast majority of the younger women have dense breasts, a great unknown number of them are potential breast cancer cases because of this- but no one has that data because mammograms don't happen as a standard until 40. Thanks to this collaboration technology (web & video conferencing), we have the advantage to reach everyone out there more easily. We're called GEN-Z... and that's the best thing about reaching my generation because everyone on my end is on Instagram, on Twitter, Facebook-- essentially web-connected. It's a whole new world that we can access and we
have to know how to use it effectively in that manner. My interest is to reach out, engage and offer true awareness to the younger women- the underserved women who have no idea about GETTING CHECKED NOW! (See Allie's spotlight feature on Earlier Detection) ROBERT BARD, MD: Speaking of generations, for us to help the underserved, we need to educate the older generation of doctors who are by and large not particularly interested in change. Use of non-invasive imaging technologies like 3D ultrasound and elastography are coming up to greatly help with early detection- instead of just a mammogram. There's an interesting link between dense breast and inflammatory disease and cancer. Meanwhile, we need more data on breast cancer cases within the younger women's age group (20-39) and there isn't any because there's no real push to get a mammo for this generation. With people like ALLIE speaking out about getting more screening, you'll find that data drive a shift in attitude as far as early detection for her age group! (See Dr. Bard's report on "The Risk of Being "Too Young for a Mammogram")
ROBERT BARD, MD: Speaking of generations, for us to help the underserved, we need to educate the older generation of doctors who are by and large not particularly interested in change. Use of non-invasive imaging technologies like 3D ultrasound and elastography are coming up to greatly help with early detection- instead of just a mammogram. There's an interesting link between dense breast and inflammatory disease and cancer. Meanwhile, we need more data on breast cancer cases within the younger women's age group (20-39) and there isn't any because there's no real push to get a mammo for this generation. With people like ALLIE speaking out about getting more screening, you'll find that data drive a shift in attitude as far as early detection for her age group! (See Dr. Bard's report on "The Risk of Being "Too Young for a Mammogram") ROBERTA KLINE, MD: Since its inception, this group has always amazed me with its vision to unite change-makers and visionaries. After all, cancer is not won from one battle front but from many. Now, we are clearly seeing an age group in crisis where cancer continues to rise simply because of a lack of attention. Allie's age group is actually first to be affected because of a lack of education and awareness, compounded by the socio-political challenges of insurance coverage and outdated practice guidelines for the medical community that perpetuate the belief that breast cancer does not happen under 40. Of course, this is far from true- but (like Dr. Bard mentioned), it's the DATA that the world listens to. So, if everyone subscribes to a data-driven approach with regular screening and personalized care, we'll change course for Allie's generation. Congratulations, Allie-- welcome to the fight! We are with you! (See Dr. Kline's report on Epigenetic Research & Profiling the Dense Breast Paradigm)
ROBERTA KLINE, MD: Since its inception, this group has always amazed me with its vision to unite change-makers and visionaries. After all, cancer is not won from one battle front but from many. Now, we are clearly seeing an age group in crisis where cancer continues to rise simply because of a lack of attention. Allie's age group is actually first to be affected because of a lack of education and awareness, compounded by the socio-political challenges of insurance coverage and outdated practice guidelines for the medical community that perpetuate the belief that breast cancer does not happen under 40. Of course, this is far from true- but (like Dr. Bard mentioned), it's the DATA that the world listens to. So, if everyone subscribes to a data-driven approach with regular screening and personalized care, we'll change course for Allie's generation. Congratulations, Allie-- welcome to the fight! We are with you! (See Dr. Kline's report on Epigenetic Research & Profiling the Dense Breast Paradigm) M.J. SMITH: Earlier detection sounds in line with my personal and professional missions. If I could wave a magic wand right now and make one single change to how we look for breast cancers, it would be to get, every woman to have a baseline mammogram at age 20. And then, in different intervals, depending on family history and breast density, 40 is that age where starting screening was established. We don't have real information available when young women may actually get breast cancer? It's devastating. They're often sent away saying, "you know, you felt this lump... you're too young to get breast cancer". There's definitely a perception issue in the medical community because of the organizations that are giving them these guidelines-- and insurers are paying only starting at age 40. There's also some exciting information coming out of AI applied to mammography and ultrasound, which are two ways that you can screen for breast cancer. AI is also helping us to determine which types of that tissue are more risky. (See MJ's spotlight video interview on Women's Health Digest about Earlier Detection)
M.J. SMITH: Earlier detection sounds in line with my personal and professional missions. If I could wave a magic wand right now and make one single change to how we look for breast cancers, it would be to get, every woman to have a baseline mammogram at age 20. And then, in different intervals, depending on family history and breast density, 40 is that age where starting screening was established. We don't have real information available when young women may actually get breast cancer? It's devastating. They're often sent away saying, "you know, you felt this lump... you're too young to get breast cancer". There's definitely a perception issue in the medical community because of the organizations that are giving them these guidelines-- and insurers are paying only starting at age 40. There's also some exciting information coming out of AI applied to mammography and ultrasound, which are two ways that you can screen for breast cancer. AI is also helping us to determine which types of that tissue are more risky. (See MJ's spotlight video interview on Women's Health Digest about Earlier Detection) JOE CAPPELLO: Allie! It's great to have you on board because you represent a
multitude of new patient groups. When
we're talking about cancer detection for a younger generation, it is amazing how many
people you're gonna affect. And your voice is very important for our mission. It's something to to behold because there's not
a lot of strong women like yourself who's willing to step out and represent a
vast majority of women who are hurting, but are afraid to come forward and
maybe not even know. But the assumption is that they should
know... and that's your voice! We've come a long way with "Are you Dense?" We do a lot off shooting in the dark, not
knowing which way to go- but in the end, we
knew we're making progress for the last 20 years. All we do
is to keep moving forward. (See: Joe Cappello's feature on Dense Breast Legislation 2023)
JOE CAPPELLO: Allie! It's great to have you on board because you represent a
multitude of new patient groups. When
we're talking about cancer detection for a younger generation, it is amazing how many
people you're gonna affect. And your voice is very important for our mission. It's something to to behold because there's not
a lot of strong women like yourself who's willing to step out and represent a
vast majority of women who are hurting, but are afraid to come forward and
maybe not even know. But the assumption is that they should
know... and that's your voice! We've come a long way with "Are you Dense?" We do a lot off shooting in the dark, not
knowing which way to go- but in the end, we
knew we're making progress for the last 20 years. All we do
is to keep moving forward. (See: Joe Cappello's feature on Dense Breast Legislation 2023)