Health issues are often linked to a range of emotional distress, but a major contributor to the progression of chronic issues such as urinary incontinence starts with the sufferer's instinct to conceal the problem. This reactive response from embarrassment and shame drives many women (both men and women) to hide their condition from their closest supporters as well as their physicians, making incontinence go unchecked and unaddressed. Over time, it is this level of clinical neglect that brings bladder health issues and urinary incontinence to grow into a more challenging health condition.[1]
Internalizing reactive shame plays a critical role in the effects of STIGMA and its self-propelling negative cycle, further driven by self-esteem issues, depression and hopelessness. From a 2002 World of Psychiatry report, both public and self-stigma may carry three components: stereotypes, prejudice, and discrimination. These elements are observed to be quite powerful in driving human activity and decision-making as they align with our sense of social acceptance, personal safety and survival.[2]
There have been many studies evaluating groups of sufferers of urinary incontinence directly reflecting emotional distress. Under varying conditions of functional loss, the investigative teams in these studies tend to conclude similar association between this physical impairment and levels of anguish and anxiety where the embarrassment of incontinence would often lead to self isolation- where seeking direct care or proper counsel is often compromised.[3]
INTRODUCTION: In my experience as an ObGyn, urinary incontinence is the unspoken secret among women. It affects up to 1 in 4 women, and this increases with age so that by age 65 up to 75% of women are affected [1]. And yet, most women never seek help. In a study published in 2013, 95% of women reported a negative impact on their quality of life, and yet 64% of the women had never received any medical help [2]. So often hidden out of shame, many women suffer in silence despite many efforts to raise awareness. Even those that are aware there is help may not seek it. What’s the point of speaking up when you fear it will only lead you down a path full of embarrassing conversations, invasive testing or procedures– and often does not produce effective or long-lasting results?
THE 'UNSPOKEN FEMALE DISORDER' While urinary incontinence is most common in women over age 50, it can happen to women of all ages. More recent research is also showing that ethnicity plays a role. Sometimes the cause is temporary, as can happen with a urinary tract infection. Pressure on the bladder, as we see in pregnancy or from fibroids or other pelvic masses, can also lead to incontinence. Addressing the underlying issue typically leads to resolution of the urinary leakage.
But most commonly, the involuntary loss of urine is not so easily fixable. The causes of urinary incontinence are grouped into four different categories: urgency, stress, functional and overflow incontinence. Functional and overflow incontinence are typically due to non-bladder related causes, while urgency and stress incontinence are closely linked with dysfunction of the bladder or other structures in the pelvic floor.
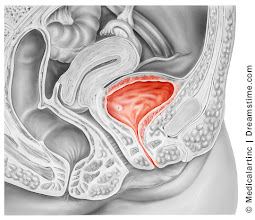
The bladder is a sac made up of smooth muscle, and when it fills up with urine there is a reflex that results in release of that urine. Early in life we learn to control when those muscles contract, and thus control when we urinate.
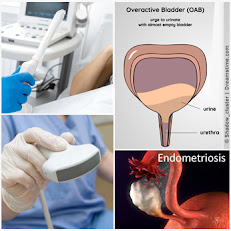
URGENCY INCONTINENCE occurs when there is some loss of that control (3). This is often called “overactive bladder”, or OAB. Certain substances, such as caffeine or wine, or changes in hormones related to menopause, are known to aggravate this. But most often, we don’t know why this occurs. As a result, lifestyle or medication treatments are often less effective because we aren’t addressing the root cause.
STRESS URINARY INCONTINENCE is most often caused by trauma to the pelvic floor during childbirth, when the muscles that are designed to support the bladder are weakened (3). As a result, women leak urine when the bladder is put under pressure such as with coughing, sneezing, laughing or jumping. This is fairly common immediately after vaginal delivery, and many women will notice their symptoms improve with Kegel exercises designed to strengthen these pelvic floor muscles, along with the natural healing process. In my experience, many women are not sufficiently educated and supported in this. Or, as is especially the case with new moms, they are so busy taking care of everyone else that they neglect their own health needs.
Some women never fully recover, and even those that do often see the stress incontinence symptoms return later in life. And to make things even more challenging, often women have both urgency and stress incontinence. So women hide, often arranging their whole lives around avoiding leaking urine because they are ashamed to seek help. They change their exercise routine. They forego activities that bring them joy and pleasure, including sex. They buy pads and hope no one notices. They are always worried about a leak that reveals their shameful secret.
In my opinion, it’s part of a larger problem in how we view and treat women’s bodies. But fortunately, things are starting to shift thanks to technological advances in both our understanding and treatment. Even Personalized Medicine is yielding breakthrough insights into underlying causes. We are learning how each woman’s DNA related to pelvic floor muscles and collagen, and the DNA of her urinary microbiome, can impact her risk as well as the effectiveness of current treatments.
I am optimistic we may someday soon be able to truly tailor both prevention and treatment in a way that is much more accessible and effective in addressing urinary incontinence in women.
Why I wear Pull-Ups… By: Jesi Stracham
When Depends became too baggy after my weight loss causing leaks and the pads would slide to the side, I switched to GoodNites brand children’s diapers. Immediately, my confidence was boosted with the cute designs and panty like fit. Even though I have my bladder well managed, I still wear them daily. With my active lifestyle I like the piece of mind that if I have an accident my wheelchair cushion and clothes will still be dry. I simply rip the diaper off, clean my downstairs “area” with a baby wipe, put a new diaper on and wheel on my way.
Often times SCI survivors suggest Botox Injections and pharmaceuticals to help with my incontinence. I used both up until April 2017 when they quit working. I searched high and low for natural alternatives after realizing how well my body felt after getting off of the pharmaceuticals. The uncomfortable constipation and dry mouth ceased within days!
Early summer 2018 I had a bladder study done. The nurse who perform the study shamed me for refusing to take the prescribed medicines. She put me in tears saying due to the amount of spasms my bladder has shrunk significantly. She continued on with a shame train because I refused pharmaceuticals after explaining they didn’t work and made me feel funny. She placed fear deep within my soul threatening that I would need a permanent catheter in my stomach with a bag or bladder augmentation (surgery where they take a piece of your bowel to make you bladder bigger) before I knew it. (see complete Blog entry)
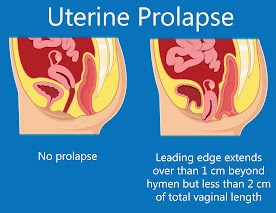
Prolapse of the pelvic floor contents (the uterus, bladder or the anus) is also associated with incontinence. 3-D pelvic floor ultrasound is performed in two ways:
1) transvaginal probe which goes inside the vagina
2) transperineal scan which is a more common way for evaluating stress urinary incontinence since the trans perineal probe is applied at the outside of the pelvic floor in the area between the vagina and the anus which is called the perineum.
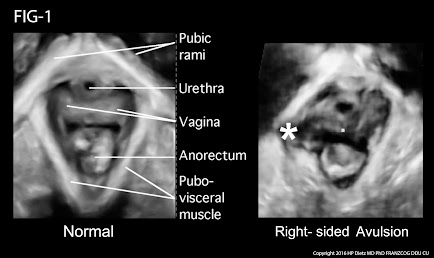
MRI has been used for years to image the prolapse of the pelvic organs but is being replaced by the 4D real time transperineal sonogram as it is quicker and instantaneously shows the tear in the muscular ring (levator sling) that is associated with the trauma of birth. This exam is done in the privacy of an office instead of an MRI center or hospital setting and may be completed in a few minutes by the physician or specially trained technician. The muscle bundle that supports the bladder is white on the sonogram while the tear is black and readily distinguished. During the examination the patient participates actively by bearing down or straining (Valsalva maneuver) to provide an exact measurement of the degree of the descent of the uterus, urethra, bladder or rectum.
THERAPY
Stress urinary incontinence (SUI) is distinct from overactive bladder (OAB) while both may be problematic in older patients with weaker muscle tone. The KEGEL maneuver is a common therapeutic approach to improve muscle strength and diminish the loss of urine when coughing, sneezing or laughing. While the technique is simple, the learning curve is often difficult for women who are accustomed to bearing down rather than “sucking up” the anus or vagina. While 4D ultrasound is optimal for diagnosing the cause, it is sophisticated equipment and requires advanced medical skills. It can go beyond diagnosis and aid in treatment: the demonstration of the bladder change in the proper Kegel contraction is visible to the patients as a dynamic training guide by the physical therapist.
The bladder descends during the Valsava while the bladder and urethra move upward in the correct maneuver. This equipment is portable so it may be brought to the patient rather than a clinic visit or a treatment facility. The technology is also wireless and point of care (POC) images may be transmitted to a reading site for interpretation as is done in ambulances where the EKG is read remotely by the Emergency Department physician while the patient is in route.
FIG-1: Postpartum delivery and difficult childbirth are a major cause of pelvic floor trauma, muscle tears and of course, urinary and fecal incontinence. The ovoid white muscular ring in this case on the right shows a star, which indicates that the white muscular lining, which is smooth on the right hand side of the picture is bulging and actually torn and disappeared by a black area, indicating the exact location at the extent of the tear. This is important preoperatively for reconstructive pelvic floor surgery. While the 3d probe takes 15 seconds to scan the entire pelvic floor surface, it takes training and of course the specialized ultrasound technology, which shows the location and the depth of the disease. More importantly, the patient dynamically assists that is active patient participation to bear down or Valsalva or hold the urine for a varied period of time is important for measuring the descent of the bladder and the uterus in the pelvic floor. Thank you very much for your attention.
For the reasons of accurate diagnosis and ease of use, pelvic floor ultrasound is widely used in Europe and becoming popular in the US. The technology is safe and a “black and white” visual aid for learning the Kegel maneuver. Additionally, during the diagnostic evaluation, the physician will look for other etiology of the voiding dysfunction such as bladder stone, bladder cancer and cystitis as well as inflammatory urethritis which is seen with treatments such as transvaginal tape (TVT) or surgical devices that are implanted. Complications of endometriosis and cervical, ovarian or uterine tumors may be detected and definitive treatment may be timely instituted.
Reference:
Dietz, H.P., Pelvic Floor Ultrasound Ultrasound, Atlas and Textbook , 2016 Obstetrics and Gynaeoclogy- Springwood NSW Australia
CONTRIBUTORS
BOBBI KLINE, MD (Educational Dir. /Women's Diagnostic Group)
Dr. Kline is a board-certified ObGyn physician, Integrative Personalized Medicine expert, consultant, author, and educator whose mission is to change how we approach health and deliver healthcare. She helped to create the Integrative & Functional Medicine program for a family practice residency, has consulted with Sodexo to implement the first personalized nutrition menu for healthcare facilities, and serves as Education Director for several organizations including the Women’s Diagnostic Health Network, Mommies on a Mission. Learn more at https://bobbiklinemd.com
ROBERT L. BARD, MD (Diagnostic Imaging Specialist)
Having paved the way for the study of various cancers both clinically and academically, Dr. Robert Bard co-founded the 9/11 CancerScan program to bring additional diagnostic support to all first responders from Ground Zero. His main practice in midtown, NYC (Bard Diagnostic Imaging- www.CancerScan.com) uses the latest in digital Imaging technology has been also used to help guide biopsies and in many cases, even replicate much of the same reports of a clinical invasive biopsy. His most recent program is dedicated to the reporting of mental health diagnostic and innovative solutions including the use of modern neuromagnetic technologies and protocols in his MEDTECH REVIEWS program.
JESSICA CONNELL-GLYNN, LCSW, CPC, CEC - (Mental Health Dir.)
As a therapist and mental health coach for the Women's Diagnostic Network, Jessica's expertise is highly in-demand in many areas of pre/post procedural care. She provides direct support in managing personal anxiety, panic, targeting TRAUMA and residually related fear. This is specialized work honed by her extensive experience and research with the general public and within the Women's Wellness community. Jessica is also currently leading an interdisciplinary research project with a team of mental health and professionals in neurology, assessing psychological disorders. (Visit her website- www.jagtheracoach.com
JESI STRACHAM is a trauma survivor on a mission to help individuals see the opportunity in their obstacles. She is the founder of Wheel With Me Foundation, the owner of Wheel With Me Consulting, and a fitness and growth coach. Through her struggles, she works for teaching individuals the power of our mindset. Jesi is an honest, authentic, America-loving athlete. Over the past several years, she has generated a significant following among both the spinal cord injury and able-bodied community. Her goal is simple: show the world there is an opportunity in their obstacles, restoring hope during life’s difficult moments. She helps people achieve their dreams through the importance of goal setting, taking control of what we have control over, and showing YOU what’s possible with consistent hard-work.
2024 CLINICAL PROFILE OF THE DENSE BREAST PARADIGM - for the Obstetrics & Gynecology Society
Breast cancer affects the lives of hundreds of thousands of women every year and is a leading cause of death. While we have made great progress in advancing earlier diagnosis and more individualized treatments, we still need to improve our approach to achieve our ultimate goal - prevention. This requires a deeper understanding of the molecular mechanisms and the multitude of factors that contribute to the development of breast cancer.
Dr. Roberta Kline, recognized speaker and publishing crusader for women's health brings you a comprehensive review and a deep-dive analysis of the current research findings about breast density and its major risk factors for breast cancer. Her reports uncover current imaging practices and clinical protocols updated in great support of breast density detection and the means of addressing this growing condition that affects over 45% of the female population. "Knowing a woman has greater breast density is a critical first step, but it doesn’t end there... we need to go further by understanding the causes of breast density, and how they relate to breast cancer-- we now have another avenue to proactively intervene to reduce risk or even prevent breast cancer in the first place." This textbook is a champion in targeting the Dense Breast Paradigm as a blueprint and a clear course study for all clinical professionals who are dedicated to women's early detection and prevention programs.(More information)
LAUNCHING IN 2024: NATIONAL COALITION OF WOMEN'S HEALTH SUPPORT
Professional health orgs, foundations and advocates of women's health disorders (primarily cancers) is uniting to form a national alliance of collaborators. This collective group is focused on "doing more together" as far as exploring new resources, sharing current ideas and addressing a wide range of topics about women's issues. Meetings like our latest Women's Powermeet series discussed the latest in diagnostic and therapeutic solutions while introducing who's who in national crusadership in the advocacy realm. Clinicians are also welcome to discuss patient-dedicated road maps and a more thoughtful health analysis and research-based evaluation. It is this level of commitment to women's health that provides a deeper sense of care for the patient that lends itself to a more holistic and integrative strategy to therapeutics. It is also this philosophy that draws more intuitive and insightful awareness on a global scale to offer collaboration platforms too better share insights on a patient's disorders to seek out better solutions. (See Women's Health Digest)
Disclaimer: The information (including, but not limited to text, graphics, images and other material) contained in this article is for informational purposes only. No material on this site is intended to be a substitute for professional medical advice or scientific claims. Furthermore, any/all contributors (both medical and non-medical) featured in this article are presenting only ANECDOTAL findings pertaining to the effects and performance of the products/technologies being reviewed - and are not offering clinical data or medical recommendations in any way. Always seek the advice of your physician or other qualified health care provider with any questions you may have regarding a medical condition or treatment and before undertaking a new health care regimen, never disregard professional medical advice or delay in seeking it because of something you read on this page, article, blog or website.

 Health issues are often linked to a range of emotional distress, but a major contributor to the progression of chronic issues such as urinary incontinence starts with the sufferer's instinct to conceal the problem. This reactive response from embarrassment and shame drives many women (both men and women) to hide their condition from their closest supporters as well as their physicians, making incontinence go unchecked and unaddressed. Over time, it is this level of clinical neglect that brings bladder health issues and urinary incontinence to grow into a more challenging health condition.[1]
Health issues are often linked to a range of emotional distress, but a major contributor to the progression of chronic issues such as urinary incontinence starts with the sufferer's instinct to conceal the problem. This reactive response from embarrassment and shame drives many women (both men and women) to hide their condition from their closest supporters as well as their physicians, making incontinence go unchecked and unaddressed. Over time, it is this level of clinical neglect that brings bladder health issues and urinary incontinence to grow into a more challenging health condition.[1]














No comments:
Post a Comment